

By Dr. Sabrina Berdouk, peer-reviewed by Abdolghader Pakniyat
You’re midway through a crowded shift. Monitors beeping, stretchers moving, voices layered over each other in the controlled chaos we call normal. Then the doors open and everything narrows.
A parent rushes in, eyes wide with fear, holding a child who is still seizing.
And in that instant, the noise fades, the room sharpens, and the only thing that matters… is the clock.
At 1 minute, everyone hopes it will stop.
At 3 minutes, you start preparing.
At 5 minutes, hope is no longer a plan.
At 5 minutes, for generalized convulsive seizures in kids, this is status epilepticus.
And the clock is now against the brain.
What Do We Actually Mean by Status Epilepticus?
Modern definitions are brutally practical:
- Seizure ≥5 minutes
- OR recurrent seizures without return to baseline
Two biological time points matter:
- t1 ≈ 5 minutes → treatment must start
- t2 ≈ 30 minutes → risk of permanent neuronal injury rises
In children, think even simpler:
A generalized tonic–clonic seizure still ongoing at 5 minutes
= treat as status epilepticus. No debate.
Why 5 Minutes Matters
Early in a seizure, inhibitory GABA pathways can still shut things down.
But as minutes pass:
- GABA receptors internalize → benzodiazepines become less effective
- Excitatory glutamate activity increases → seizures self-sustain
- Cerebral metabolism, hypoxia, acidosis, and hyperthermia rise
- Neuronal injury risk accelerates toward the 30-minute mark
So refractory status epilepticus often doesn’t start in the ICU.
It starts with delayed or underdosed treatment in the first 10 minutes.
Minute 0–5: The Moment That Changes Everything
Your priorities are simple:
Airway. Breathing. Circulation. Glucose. Access. Monitoring.
Then the intervention that still determines outcome more than any other:
A full, weight-based benzodiazepine.
Given early. Given properly. Given once… and repeated once if needed.
Not a symbolic dose.
Not scattered mini-doses.
Not hesitation.
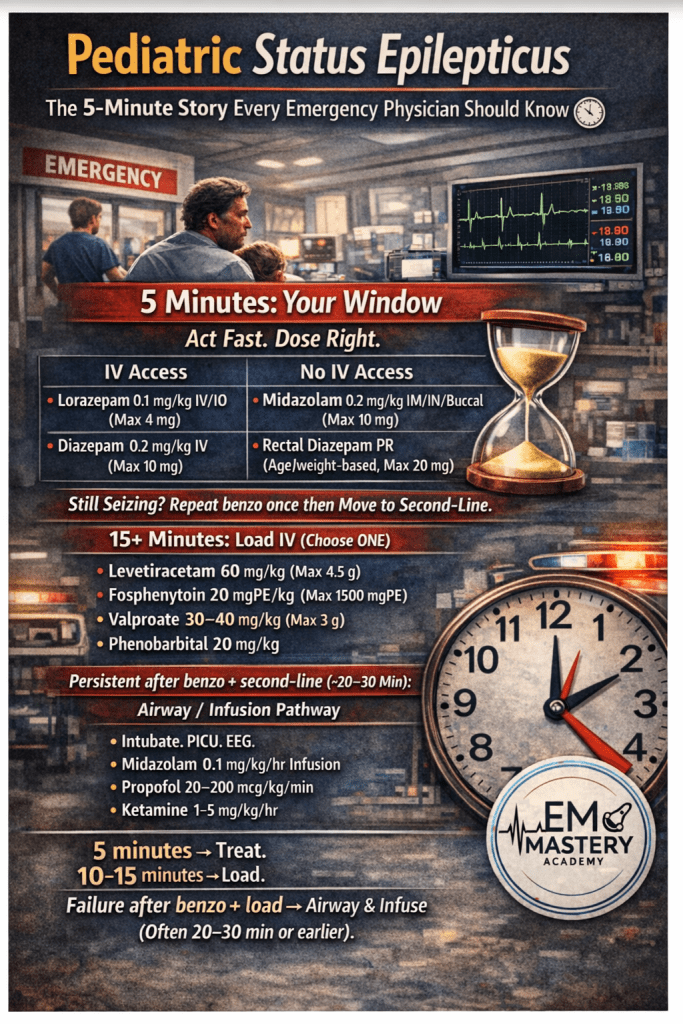
| IV Access | No IV Access |
|---|---|
| Lorazepam 0.1 mg/kg IV (max 4 mg) | Midazolam 0.2 mg/kg IM/IN/buccal (max 10 mg) |
| Diazepam 0.2 mg/kg IV (max 10 mg) | Rectal diazepam 0.5 mg/kg ( 2-6b years old ) , consider lower mg/kg in older kids/teens ( 0.3 mg/kg kids 6-12 years old ) (max 20 mg) |
If still seizing 5 minutes after an adequate dose, repeat once.
Then something critical must happen:
You must move on.
Minute 10–30: Where Systems Beat Intentions
What should happen next is clear:
One full second-line IV loading dose. Immediately.
- Levetiracetam 60 mg/kg (max 4.5 g) or
- Fosphenytoin 20 mg/kg (max 1500 mg)
- Valproate 30–40 mg/kg (max 3 g , caution children <2 years (and in suspected mitochondrial disease/POLG risk))
- Phenobarbital 20 mg/kg (infants or contraindications). Not our favorite… for obvious reasons….
Different drugs.
Similar efficacy ; choose based on contraindications and speed-to-delivery.”
What truly determines outcome is:
Speed. Dose. Decisiveness.
Because across pediatric SE audits worldwide, the most consistent delay is not pharmacology.
It’s hesitation.
If still seizing after adequate benzo(s) + a full second-line load, prepare airway/continuous infusion (often ~20–30 min, sometimes earlier) , you need to escalate to the next step …..
Beyond 30 Minutes: When the Definition Changes Again
Persistent seizures now mean:
Refractory status epilepticus.
Management shifts from intermittent pushes
to continuous control:
Intubation. Ventilation. Continuous EEG. PICU.But who has an EEG in their ER…..?
Continuous anesthetic infusion.
Common pediatric infusion strategies:
- Midazolam:
- Bolus 0.2 mg/kg IV
- Infusion 0.1 mg/kg/hr, titrate up (≈ 0.3–2 mg/kg/hr) to seizure or burst suppression
- Propofol (older children, selected/short-term):
- Roughly >8–10 years, especially teens
- Bolus 1–2 mg/kg IV
- Infusion 20–200 mcg/kg/min
- Monitor for propofol infusion syndrome, avoid prolonged high doses. Actually great agent for induction.
- Roughly >8–10 years, especially teens
- Ketamine or barbiturate infusion (e.g., pentobarbital/thiopental)
- Used per PICU protocol when seizures persist despite the above
And while the seizure is controlled, the real question begins:
Why did this child seize?
Infection.
Electrolytes.
Toxins.
Trauma.
Autoimmune disease.
Hypoxia.
Medication levels.
Stopping the seizure is lifesaving.
Finding the cause is future-saving.
The Pitfalls We Still See — Even in Excellent Departments
Not from lack of care.
But because emergency medicine is human.
- Waiting past 5 minutes
- Underdosing benzodiazepines
- Repeating benzos instead of escalating
- Delayed second-line loading
- Missing reversible causes
- No clear time-based bedside pathway
These are not knowledge failures.
They are system failures.
And systems can be fixed.
The Quiet Truth
Outcome in pediatric status epilepticus is often decided:
Before neurology arrives.
Before EEG.
Before ICU.
It is decided in the first 10 minutes
by the emergency team
choosing whether to move fast enough.
The Take-Home
5 minutes → Treat.
10 minutes → Load.
Failure of benzo + second-line load → airway/infusion pathway (often ~20–30 min or earlier) → Intubate and infuse.
No hesitation.
No underdosing.
No delay.
Because in pediatric status epilepticus:
Speed protects brains.
Precision protects futures.
By








