
The key question is not “Is the QRS changing?”

The key question is:
Is the QT interval prolonged or not?
That single distinction changes the physiology, the cause, and the treatment.
Polymorphic VT in one sentence
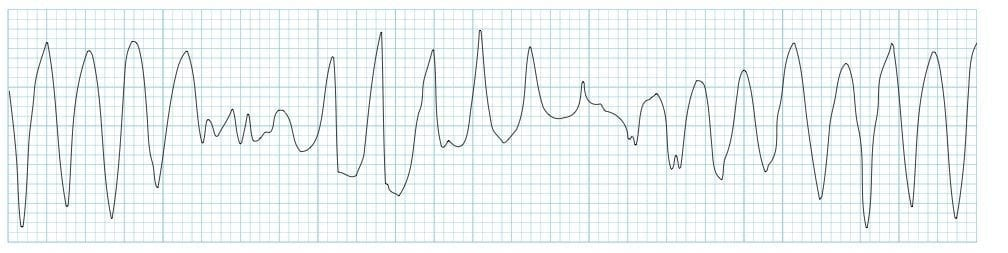
It may:
- stop on its own and come back,
- become sustained,
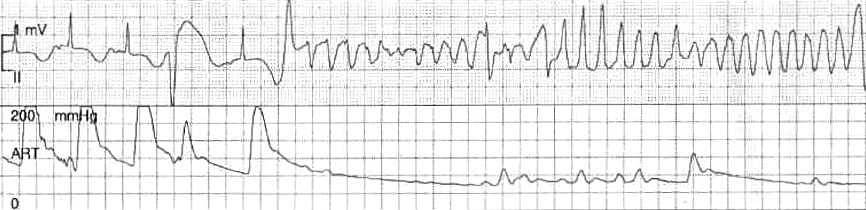
- or degenerate into ventricular fibrillation (VF).
In fact, VF often starts as polymorphic VT, and prolonged pVT often becomes VF.
The bedside rule
Polymorphic VT = unsynchronized shock
Unlike monomorphic VT, you usually cannot reliably synchronize because the QRS keeps changing.
So the electrical treatment is:
High-energy unsynchronized shock (defibrillation)
Not synchronized cardioversion.
Two major clinical classifications
1) Polymorphic VT with prolonged QT = torsades de pointes
This is the classic form everyone remembers.
Why it happens physiologically
A prolonged QT means delayed ventricular repolarization.
That creates electrical instability and allows early afterdepolarizations, which can trigger torsades.
It is more likely when:
- QTc > 500 ms
- especially with bradycardia
- plus triggers like:
- QT-prolonging drugs
- hypokalemia
- hypomagnesemia
- congenital long QT syndromes
Clinical pattern
Torsades often comes in bursts:
- starts
- self-terminates
- recurs again and again
So even if you shock it successfully, it may come right back unless you resolve the underlying substrate.
Treatment priorities
Defibrillate if unstable or pulseless.
IV magnesium.
Aggressively correct potassium and magnesium (Target: Potassium > 4.0 mEq/L and Magnesium > 2.0 mg/dL).
Stop QT-prolonging drugs.
If associated with bradycardia/pause dependence, consider:
- Overdrive pacing.
- Isoproterenol (Caution: Isoproterenol severely increases myocardial oxygen demand. If the pVT is actually driven by hidden ischemia, it can worsen the condition and trigger fatal ventricular fibrillation).
- Expert consultation.
Important pitfall
Many antiarrhythmics can worsen torsades because they prolong QT further.
So in torsades:
- magnesium helps
- QT-prolonging antiarrhythmics may hurt
Also, acute beta-blockade can worsen bradycardia, so in pause-dependent torsades it may aggravate the problem.
2) Polymorphic VT without prolonged QT


This is a different disease until proven otherwise.
Most common cause
Acute myocardial ischemia/infarction
Physiology
This is usually not a repolarization problem like torsades.
It is more often an ischemic ventricular irritability problem—injured myocardium becomes electrically chaotic and degenerates rapidly toward VF.
Treatment priorities
- Immediate defibrillation
- Treat the ischemia
- Antiarrhythmics such as:
- lidocaine
- amiodarone
- Beta-blockers may help when ischemia is the driver
- Consider emergent coronary reperfusion when appropriate
Important pitfall
Magnesium is not useful just because the rhythm is polymorphic.
It is helpful for torsades / long-QT pVT, not for routine polymorphic VT with a normal QT.
The most important practical distinction
Torsades
Think:
- long QT
- often bradycardia/pause-triggered
- magnesium
- correct electrolytes
- pacing/isoproterenol if needed
- avoid QT-prolonging drugs
Non–long-QT polymorphic VT
Think:
- ischemia until proven otherwise
- defibrillate
- treat ACS / MI
- lidocaine or amiodarone may help
- beta-blockade may help if ischemia-driven
A memorable one-liner
In polymorphic VT, don’t focus first on the changing QRS—focus on the QT.
Because:
- Long QT → torsades → magnesium and rate acceleration
- Normal QT → ischemic pVT → defibrillation and treat ischemia
Bedside pearls
- All polymorphic VT is unstable
- It is often hard to distinguish from VF
- If in doubt and if the patient is hemodynamically unstable, defibrillate
- Shocking terminates the episode, but does not fix the cause
- Magnesium is for torsades, not for all polymorphic VT
Simple algorithm
- Recognize wide irregular ventricular tachyarrhythmia.
- Treat as unstable.
- Consider brief procedural sedation (if the patient is conscious and time permits).
- Deliver high-energy unsynchronized shock.
- Ask: Is the baseline QT interval prolonged?
- Yes (Known long QT): Think torsades → Give IV magnesium, aggressively correct K/Mg (target K > 4.0 mEq/L, Mg > 2.0 mg/dL), and remove QT-prolonging drugs. Consider pacing if bradycardic.
- No (Known normal QT): Think ischemia → Treat acute coronary syndrome (ACS), consider lidocaine or amiodarone, and use beta-blockers when appropriate.
- Unknown baseline QT: Default to treating as ischemic pVT (which is statistically more common), but give empirical IV magnesium, as it carries a low risk profile and covers potential torsades.
Bidirectional VT deserves special mention.
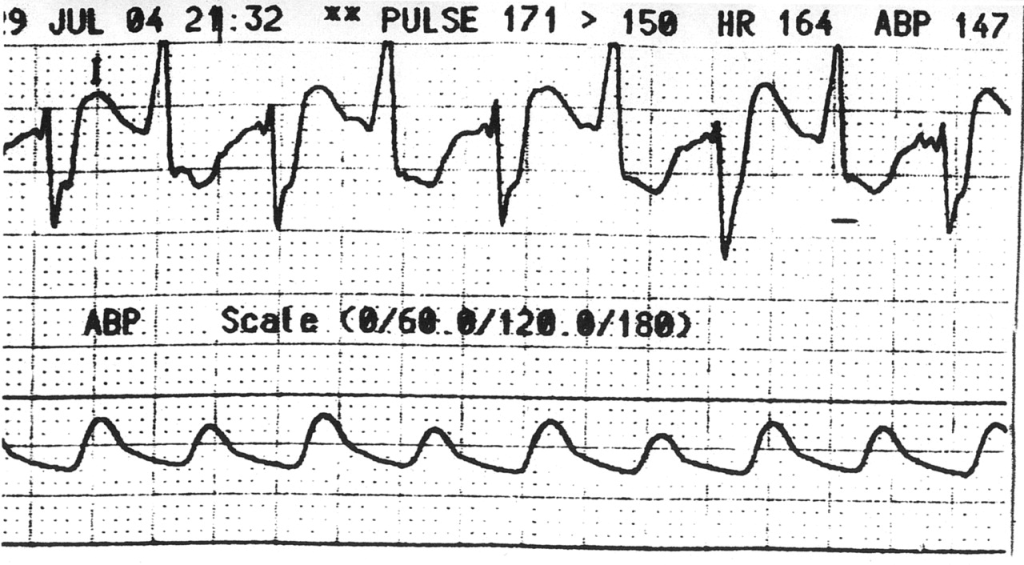
It is a distinctive form of ventricular tachycardia where the QRS axis or morphology alternates from beat to beat. Unlike classic torsades, it should immediately raise suspicion for specific diagnoses, most notably digoxin toxicity and catecholaminergic polymorphic VT (CPVT). More rarely, it can be seen in conditions such as Andersen–Tawil syndrome or myocarditis.
The clinical directive is straightforward: treat the instability first, but intervention must not cease upon terminating the rhythm. For instance, in cases of digoxin toxicity, clinicians must immediately halt the offending agent, correct associated electrolyte abnormalities, and administer digoxin immune Fab when indicated. Alternatively, in CPVT, the goal is to suppress adrenergic triggers; beta-blockers are the foundation of therapy, whereas flecainide may be added if arrhythmias persist. Ultimately, bidirectional VT is not just an ECG curiosity—it is a critical clue to the underlying mechanism that must guide your treatment.
The R-on-T phenomenon also deserves attention.

This phenomenon helps explain how malignant ventricular arrhythmias begin. It occurs when a premature ventricular beat falls directly on the T wave, meaning it arrives during the vulnerable phase of repolarization before the ventricle has fully reset. Consequently, this poorly timed impulse can trigger polymorphic VT, torsades de pointes, or even ventricular fibrillation.
Ultimately, the key point is timing; R-on-T is not a primary diagnosis, but rather a physiological trigger. When identified in the setting of a prolonged QT interval, ischemia, or an electrolyte disturbance, it warrants immediate clinical concern, as the substrate is electrically unstable and the risk of a life-threatening arrhythmia is critically high.
Final thoughts
Polymorphic VT is more than an ECG pattern. It is a sign of electrical instability. The most important question is simple: is the QT interval prolonged? A long QT points toward torsades. A normal QT points more toward ischemia or another arrhythmic substrate.
Some patterns offer even more clues. Bidirectional VT should raise suspicion for diagnoses such as digoxin toxicity or CPVT. The R-on-T phenomenon should be recognized as a trigger, not a diagnosis. It shows how a poorly timed ventricular beat can ignite a dangerous arrhythmia.
The final lesson is straightforward. Do not stop at naming the rhythm. Do not stop at terminating the episode. Check the QT. Look for the trigger. Identify the substrate. Then treat the mechanism.
By Dr. Abdolghader Pakniyat, Peer-reviewed by Dr. Sabrina Berdouk








